TREATMENTS FOR KERATOCONUS
Corneal Cross Linking
Purpose - Risks - Start of effect ccl - Procedure - Follow up - Visual rehabilitation - Conclusion
Definition of CCL
The cornea consists of collagen fibers. We use Riboflavine ( Vit B2 is fotosensitive) to create extra bands between these fibres and so strengthen the cornea. So CCL is the cross linking of corneal collagen fibres.
Mechanism of actions of CCL
 CCL has been demonstrated ex vivo to favourably influence the strength of the cornea. It has been used in vivo with good success. This is revolutionary for keratoconus patients, as even a delay (if not absolutely arrest) of the condition will markedly reduce visual morbidity as well as reduce the number who will require corneal transplants.The biomechanical basis of increased corneal strength is the formation of covalent crosslinks that occur when the photosensitiser, riboflavin, is applied to the deepitheliazed surface of the cornea and subsequently exposed to UV-A light. Free radicals created by the excitation of riboflavin at its absorption peak 370 nm are thought to interatct with amino acids in neighboring collagen molecues to form strong chemical bonds. CCL has been demonstrated ex vivo to favourably influence the strength of the cornea. It has been used in vivo with good success. This is revolutionary for keratoconus patients, as even a delay (if not absolutely arrest) of the condition will markedly reduce visual morbidity as well as reduce the number who will require corneal transplants.The biomechanical basis of increased corneal strength is the formation of covalent crosslinks that occur when the photosensitiser, riboflavin, is applied to the deepitheliazed surface of the cornea and subsequently exposed to UV-A light. Free radicals created by the excitation of riboflavin at its absorption peak 370 nm are thought to interatct with amino acids in neighboring collagen molecues to form strong chemical bonds.
Purpose
By the use of this technique, we flatten the cornea and the patient will better tolerate his contactlenses. It can postpone or even prevent an eventual corneal graft. The corneal surface becomes more regular. Long term, we are still uncertain whether a need for repeat procedures will arise because of natural collagen turnover: follow up is needed to measure the durability of the strengthening effect. Repaet treatments may be necessary to prevent recurrence of disease progression. Time will tell of the long-term durability during the yearly eye examination by corneal topography.
Other indications for CCL
Pellucid marginal degeneration
Corneal ectasia after refractive surgery
Forme fruste of keratoconus
Corneal deformation after radial keratotomy
Contraindications
Corneal epithelial healing disorders
Refractive keratotomy
Previous herpes keratitis
Corneal melting disorders
Pregnancy
Risks of CCL
Very low risk profile
Haze which is uncommon and easily managed with topical steroids
Delay in reepithelialisation
Infection
Sterile infiltrates
Potential of induction of Herpes keratititis
Ocular surface disorder and tear dysfunction
Up until today no sight threatening side effects have been reported.
Start of effect crosslinking
Begins after 30 min of application UV-A
Continues during months
It may take 3 to 6 months before ready to be fitted for contact lenses
Our own reports to date confirm effectiveness in stabilizing corneal biomechanics and rehabilitating patients without the need for more invasive procedures.
In most of the cases the evolution of keratoconus stopped and the cornea may flatten up to 4 diopters
Procedure
 The intervention is carried out on a ambulatory basis in the eyecenter inKortrijk or St-Martens-Latem under topical anaesthesia. It takes about 90 min under aseptic conditons in an operation theatre with airfiltration by laminar air flow. First the superficial epithelial layer of the cornea is removed ( this will recover in 5 days). The intervention is carried out on a ambulatory basis in the eyecenter inKortrijk or St-Martens-Latem under topical anaesthesia. It takes about 90 min under aseptic conditons in an operation theatre with airfiltration by laminar air flow. First the superficial epithelial layer of the cornea is removed ( this will recover in 5 days).
Than the cornea ispresaturated with the riboflavine for 30 minutes. The eye surgeon will than check at the slitlamp if the dye has sufficiently penetrated the cornea after which the irradiation w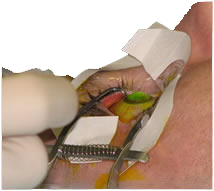 ith UV light ( 365 nm) can be applicated to the corneal surface for about 30 minutes. Regular application of riboflavinduring irradiation enhances safetyprotecting the deeper endothelium, lens and retina by absorbing the UV-A light source. ith UV light ( 365 nm) can be applicated to the corneal surface for about 30 minutes. Regular application of riboflavinduring irradiation enhances safetyprotecting the deeper endothelium, lens and retina by absorbing the UV-A light source.
A bandage contact lens is applied for 5 days. The patient is instructed to applicate antibiotic drops and natural tears for at least 2 weeks after CCL. Topical steroids are tapered over the next months. Individual tolerance to pain and light sensitivity is highly variable; if necessary use of paracetamol can be necessary and accounting for days off work.
Follow up
Bandage contact lens can be removed after 5 days
Patient can return to work after 5-10 days
In the beginning glasses if possible has to be used
After 6 weeks the original contact lenses can be used
New contact lens adaptation not earlier than 3-6 months after CCL
If final visual acuity is not sufficient intracorneal ring segments are possible
Yearly serial topography is important to chart progress or recogize postop regression if and when it should occur.
 Visual rehabilitation Visual rehabilitation
CCL is a routine treatment to keratoconic patients.
After 3-6 months the visual
acuity and topography had to
be checked. If the visual acuity
is insufficient with gas permeable contact lenses, intracorneal ring segments had to be placed to flatten the cornea more.
These treatments diminish
the need for lamellar of
penetrating keratoplasty.
Conclusion
Corneal Cross Linking is
currently the best and only
option to stop or minimize the progression of ectatic corneal diseases.
|
